Even though the COVID-1 9 mortality bow has been flattened, mainstream media stores continue to push doomsday predictions of an impending detonation of deaths. The New York Times, for example, wrote essays July 21,2 and July 3,3, 4 2020, basically forewarning everyone to not get excited about plummeting death paces, as the trend could change at any moment.
“Why Virus Deaths Are Down but May Soon Rise, ” its July 2 headline territories. The commodity goes on to claim “coronavirus trends in the United States are pretty dark right now” — based on surging case digits, entailing positive research makes , not hospitalizations or people exhibiting actual indications.
The article attributes the steady and relatively rapid drop-off in demises to improved medical treatment and older people being more cautious, but warns that “Deaths may be on the brink of rising again, ” because “middle-aged and younger people are acting as if they’re invulnerable” and has been rising their social undertakings.
“Their increased social pleasure has fueled an detonation in cases over the last three weeks, which in turn could lead to a rise in extinctions soon, ” The New York Times states, 5,6 contributing 😛 TAGEND
“With testing now more widespread, it’s possible that the demise data will lag the action data by closer to a month.( In a normal fatal action, the fatality comes three to five weeks after constriction of the virus .) If that’s correct, coronavirus deaths may start rising again any day.”
This, however, entirely neglects data showing that the COVID-1 9 fatality rate for those under persons under the age of 45 is “almost zero, ” and between the senilities of 45 and 70, it’s somewhere between 0.05% and 0.3%. 7,8, 9
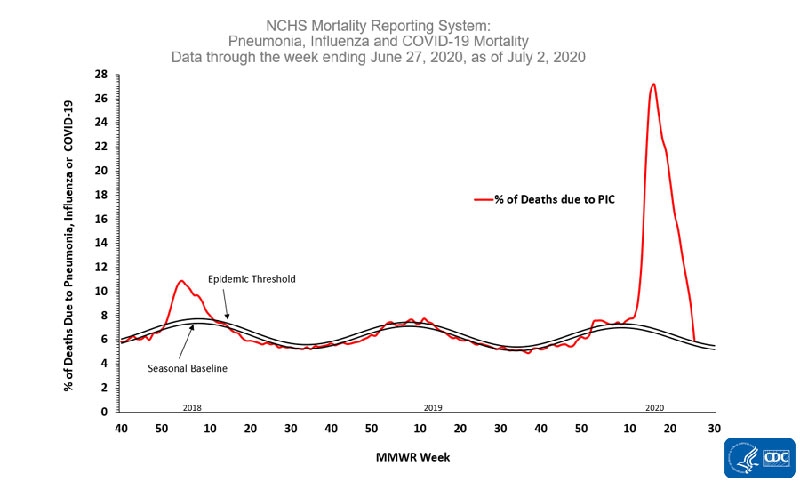
COVID-1 9 mortality — which had waned for the last 10 weeks straight-out — is currently at the epidemic threshold, meaning if it slips down merely a little more, COVID-1 9 will no longer meet the CDC’s criteria for “epidemic” status.
In other utterances, the facts of the case that young and middle-aged adults are measuring positive in droves is not a warning sign of an impending foray of deaths, as the risk of extinction in these age groups is minuscule. If anything, it seems to show herd exemption is building which, eventually, will help protect the most prone among us.
Why Did They Want to Flatten the Curve?
The primary justification for the inhuman administrative involvements of COVID-1 9 was to slow the spread of the illnes so that hospital aids would not be devastated, motiving people to die due to lack of medical care. These involvements were not about stopping the spread or reduce the amount of people that would eventually get infected.
It was only intended to slow it down so, eventually, naturally-acquired herd immunity — the best kind — would prevent its spread. Well guess what? They have changed the narrative. That is why you now do not hear anything about dropping the bow. Instead they transitioned the fear-mongering to startle the public that the number of “cases” are increasing.
Bear in attention that you do NOT need any experiment to be classified as a COVID case. All there is a requirement is a simple upper respiratory infection and you can legally be classified as a COVID-1 9 bag to artificially inflate the totals.
Fatality Rate No Longer Cause for Hysteria
The fatality rate data given above were cited by Stanford University’s sicknes prevention chairperson Dr. John Ioannidis — an epidemiologist who has made a name for himself by uncovering bad discipline — in a June 27, 2020, interrogation with Greek Reporter, 10,11, 12 in which he criticized global lockdown sets, saying they were implemented based on flawed modeling and grossly unreliable data.
“0. 05% to 1% is a reasonable assortment for what the data tell us now for the infection fatality rate, with a median of about 0.25%, ” Ioannidis told Greek Reporter. 13
“The death rate in a reporting country depends a parcel on the age-structure, who are the people infected, and how they are oversaw. For beings younger than 45, the infection fatality rate is almost 0 %. For 45 to 70, “its probably” about 0.05 -0. 3 %.
For those above 70, it heightens greatly, to 1% or higher for those over 85. For frail, incapacitated elderly people with several health problems who are infected in rest home, it can go up to 25% during major eruptions in these facilities.”
When invited whether the swerve had indeed been dropped in the U.S ., watching how no state care organisation had been totally devastated, Ioannidis answered: 14
“The predictions of most numerical patterns in expressions of how many plots and how many ICU bunks would be required were astronomically wrong. Indeed, the health system was not overrun in any point in the USA, although several hospitals were accentuated. Conversely, the health care organization was severely damaged in countless regions because of the measures made …
Major ramifications on their own economies, civilization and mental health have already passed. I hope they are reversible, and this depends to a large scope on whether we are able to evaded prolonging the draconian lockdowns and manage to deal with COVID-1 9 in a smart-alecky, precision-risk targeted approaching, rather than indiscriminately shutting down everything …
I hope that policymakers look at the big picture of all the potential both problems and not only on the very important, but relatively thin slice of evidence that is COVID-1 9. “
COVID-1 9 Close to Epidemic Threshold
The fear-mongers also ignore recent Core for Disease Control and Prevention statements1 5 saying the COVID-1 9 death — which had rejected for the last 10 weeks straight-from-the-shoulder — “is currently at the epidemic threshold, ” meaning if it slides down only a bit more, COVID-1 9 will no longer meet the CDC’s criteria for “epidemic” status.
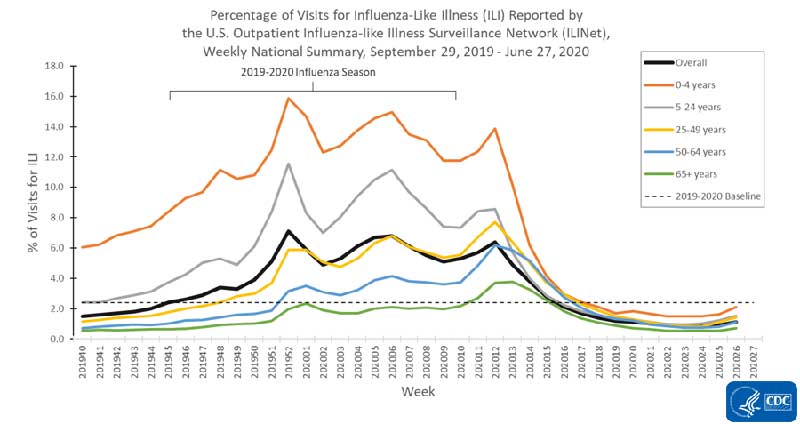
The percentage of doctors’ stays for influenza-like illness( ILI) for all age groups has also stopped below the 2019 -2 020 baseline, as seen in the CDC graph below, published July 3, 2020.16
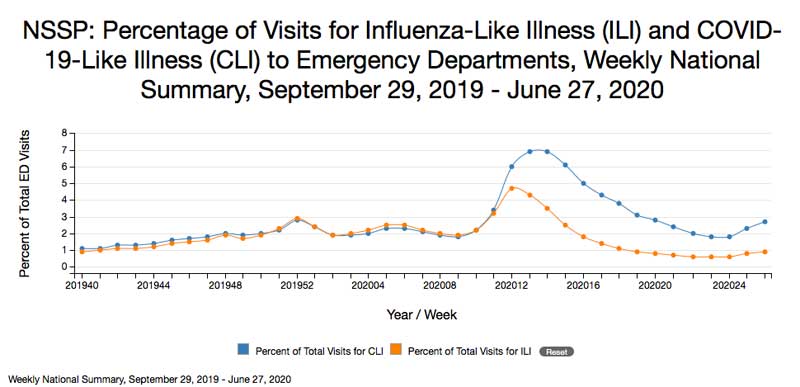
The graph below shows the percentage of visits to emergency bureaux, precisely, referred to supposed ILI and COVID-1 9-like illness( CLI ). While ER sees for suspected COVID-1 9 have looked a slight uptick, it’s not situations of extreme increase.
The Truth About Increasing COVID-1 9 Actions
The video above recalls why the rise in COVID-1 9 “cases” is misinforming at best, and not a practicable measure of a public health threat. It presents a historical overview of what happened during the 2009 swine flu pandemic, and how it parallels the current COVID-1 9 pandemic.
In summary, dread of a novel illness — pandemic swine influenza — had contributed to a stunning spike in testing, compiling it seem like a significant threat as countless be positive. Yet the deaths was insignificant. We’re seeing the same thing happening now. Two things are driving the numbers of positive assessments skyward: The abrupt accessibility of tests, and widespread testing of asymptomatic parties.
Put another method. The sharp increases in “cases” are not proof of disease spread but instead the spread of testing. When you don’t have a test for the illnes, you cannot tally positive occurrences. Hence it looked like there were virtually no COVID-1 9 events in January 2020.
The sudden hop in cases in February links with the coming of exam kits is sending out by the CDC. Once those exam equipment were used up, the number of “cases” again dried up. Then, once evaluation gears became readily available again in early April, the number of cases skyrocketed — as you’d expect. But again, this doesn’t mean the disease was spreading like wildfire.
It was probably in circulation throughout and countless people were already walking around with it, feeling no worse than normal. The only difference is that test kits became available and massive amounts of people — whether they had symptoms or not — were being tested.
Increased Testing= Increased ‘Cases’
In short-lived, the diagrams registering “cases” in large-scale duty simply illustrate the fact that there are testing. Granted, even this is an oversimplification and is not going to be accurate, and there’s more than one rationalization for this. For example, during the third week of May, the CDC admitted it had mixed the results from viral and antibody measures in its national arises. 17
This plies a certainly incorrect illustration, since the two research describe very different things. The viral measure is supposed to identify active infections( irrespective of whether “youve had” symptoms or not ), whereas the antibody test tell me something if you’ve been exposed to the virus in the past and fight it off by developing antibodies. Hence, an antibody research should not be counted as an active infection or active “case.”
Some data1 8 too suggest positive assessment reactions have worsened even as testing has increased. The question is, could this be an indication that people who are being tested for active infection have already fought off the virus and have antibodies? Could it be a sign of rising flock exemption?
Unfortunately, COVID-1 9 test data has been so mishandled and the room the data is compiled has converted enough times that it’s virtually impossible to make sense of it at this detail. The aspect and reliability of the tests themselves, both viral and antibody, too appear to be less than stellar.
The CDC has admitted that prior showing to coronaviruses is accountable for the common cold can lead to a positive COVID-1 9 antibody evaluation, 19 and during an April White House Coronavirus Task Force briefing, Dr. Birx explained that COVID-1 9 measures are “not 100% sensitive or specific, ” and that when prevalence is low in the community, the fictitiou positive pace will be high.
“If you have 1% of your population fouled, and you have a test that’s exclusively 99% specific, that makes that when you find a positive, 50% of the time will be a real positive and 50% of the time it won’t be, ” Birx said. In other messages, if the prevalence of infection in their own communities is 1 %, approximately half of all positive experiments will be false positives.
Only as the overall infection rate gets higher does the viral research become increasingly reliable. Who knows, perhaps this is why some of the data indicate the number of positive measures is actually weakening even as testing continues to rise?
What Happened to the Death Toll Reporting?
As you are eligible to remembrance, earlier today, the media focused on the death toll and hospitalizations. We had daily bulletin ticker videotapes plying us with the numbers of severe and critical occurrences, and the number of deaths.
These statistics were used to justify draconian lockdown requires to prevent hospitals from becoming overwhelmed. Now you examine virtually nothing about hospitalizations or deaths.
It’s all about the rising number of “cases, ” meaning infected individuals, which is to be expected when you test a population in which the virus has already infected the majority. But that doesn’t mean it poses a threat, since demises continue to descend.
It seems numerous are simply unwilling to accept the good news and allow the population to return to regular living. Instead, “rising cases” — especially among previous low-risk age group — is now being used to justify continued stay-at-home orderings, even though hospitals are at no risk of being devastated since a vast majority of these cases are asymptomatic and need nothing in terms of health care.
In its April 13, 2020, matter, the German magazine Blauer Bote2 0,21 lists a collection of 75 expert beliefs about the COVID-1 9 threat. Among them is a statement from Gerd Bosbach, 22 prof emeritus of statistics, mathematics and empirical economic and social research, and generator of the book, “Lying With Numbers, ” who said( carried from German to English employ TranslationLookup.com2 3 ): 24
“The tripling of the tests resulted in a little more than tripling the number of those who tested positive. This tripling was presented to the citizens as a tripling of hiv infected …
Far-reaching decisions compel stick organizations. This is exactly what has been neglected still further. The repeated equation of the number of positively researched people with the number of infected massed the deem …
The government’s standard of when steps should be faded is based on an supposed number of polluted people, which has nothing to do with reality …
So we have a muddle of words, which is ultimately attributed to the fact that we keep talking about infected parties instead of positive beings. The high numbers remain in memory, such as the mortality rate of 3.4% stated by the WHO. And that creates fear …
We should ensure that the media do not use the supremacy of epitomes to generate ardours that are affecting our arbitration. If you get photographs of coffins and death districts from Italy or photographs of fully empty shelves, then their effects exceed the facts mentioned.”
Herd Immunity Likely Much Higher Than Suspected
In relevant information, various recent studies intimate a majority of the population may already have immunity against COVID-1 9, via one mechanism or the other. Harmonizing to a Swiss study, 25,26 SARS-CoV-2-specific antibodies are only found in the most severe cases — about 1 in 5. That recommends COVID-1 9 may in fact be five times more prevalent than supposed. This also intends it may be five times less deadly than foreseen. According to the authors:
“When symptomatic, COVID-1 9 can straddle from a mild flu-like illness in about 81% to a severe and critical disease in about 14% and 5% of changed cases, respectively.”
They also found that even though people who had been exposed to COVID-1 9 had SARS-CoV-2-specific immunoglobulin A( IgA) antibodies in their mucosa, there were no virus-specific antibodies in their blood.
IgA is an antibody that plays a crucial role in the immune gathering of your mucous sheaths, while IgG is the most common antibody that protects against bacterial and viral illness and is found in blood and other bodily fluids. As explained by the authors: 27
“As with other coronaviruses, symptomatic SARS-CoV-2 disease campaigns an acute illnes with activation of the innate and adaptive immune structures. The former leads to the release of several pro-inflammatory cytokines, including interleukin-6 …
Subsequently, B and T cadres become activated, ensuing in the production of SARS-CoV-2-specific antibodies, comprising immunoglobulin M( IgM ), immunoglobulin A( IgA ), and immunoglobulin G( IgG ).
Whereas coronavirus-specific IgM production is transient and leads to isotype switch to IgA and IgG, these latter antibody subtypes can persevere for extended periods in the serum and in nasal liquors. Whether SARS-CoV-2-specific IgG antibodies correlate with virus ascendancy is a affair of intense discussions.”
Majority of People Appear Resistant to COVID-1 9
Another study2 8,29 published in the periodical Cell determined 70% of samples from patients who had recovered from mild cases of COVID-1 9 had resistance to SARS-CoV-2 on the T-cell level. Curiously, 40% to 60% of people who had not been exposed to SARS-CoV-2 too had fighting to the virus on the T-cell level.
According to the authors, this advocates there’s “cross-reactive T cell acceptance between spread ‘common cold’ coronaviruses and SARS-CoV-2. ” In other messages, if you’ve retrieved from a common cold caused by a particular coronavirus, your humoral immune plan may initiate when you encounter SARS-CoV-2, thus yielding you resistant to COVID-1 9.
May 14, 2020, Science magazine reported3 0 these Cell conclusions, attracting parallels to another earlier paper3 1 by German investigates that has now come to a similar opinion. That German newspaper, 32 the preprint of which was posted April 22, 2020, on Medrxiv, met aid T cells that targeted the SARS-CoV-2 spike protein in 15 of 18 cases hospitalized with COVID-1 9.
Yet another study, 33,34, 35 this one by investigates in Singapore, concluded common cold caused by the betacoronaviruses OC43 and HKU1 might build you more resistant to SARS-CoV-2 infection, and that the resulting immunity might previous as long as 17 years.
The authors suggest that if you’ve beat a common cold caused by a OC43 or HKU1 betacoronavirus in the past, you may have a 50/50 opportunity of having defensive T-cells that can recognize and help defend against SARS-CoV-2.
81% of Unexposed Someone May Be Resistant to SARS-CoV-2
Two additional studies advocating herd immunity is near were reported3 6 by Reason, July 1, 2020. These include a Swedish study, 37,38 which find “SARS-CoV-2 elicits robust cache T cell responses akin to those observed in the context of successful vaccines, is proposed that natural revelation or illnes may thwart recurrent bouts of severe COVID-1 9 also in seronegative individual.” Similarly, a German study3 9 concluded 😛 TAGEND
“SARS-CoV-2-specific T-cell epitopes enabled identification of post-infectious T-cell immunity, even in seronegative convalescents. Cross-reactive SARS-CoV-2 T-cell epitopes divulged preexisting T-cell responses in 81% of unexposed individuals, and validation of similarity to common cold human coronaviruses supported a functional basis for theorized heterologous exemption in SARS-CoV-2 infection.”
Flattening the Curve Was a Fool’s Errand
So far, many efforts to curb COVID-1 9 illnes have proven to be ill cautioned. Suggestion shows the illness spreads mostly indoors, 40,41, 42 for example, throwing doubt on the stability of closing parks and seas, especially during the summer. As reported by The Baltimore Sun, 43 scientists are now considering expending ultraviolet light to eradicate SARS-CoV-2 in indoor aura. Step outside, and you get that impression for free.
The total all-cause mortality is not significantly different than in previous years as to be considered by my interrogation with Denis Rancourt. Many other extinctions have been shifted to COVID-1 9, bringing a high spike in deaths, but when you look at the country under the curve for total fatalities, it actually doesn’t differ from previous years.
This was also resembled by the American Institute for Economic Research. 44 Back in April 2020 they referred to the COVID-1 9 pandemic as “An scandalous statistical fright story” that resulted in “a vandalistic lockdown on the economy, ” which 😛 TAGEND
” … would have been an outrage even if the suppositions were not wildly astronomically wrong. Flattening the veer was always a fool’s errand that widened the damage …
The latest figures on overall death rates from all justifications picture no advance at all. Deaths are lower than in 2019, 2018, 2017 and 2015, slightly larger than in 2016. Any uphill bias is imparted by population growth.
Now writing a book on the crisis with bestselling scribe Jay Richards,[ statistician William] Briggs concludes: ‘Since pneumonia extinctions are up, yet all demises are down, it must mean parties are being recorded as dying from other things at smaller frequencies than usual.’ Demises from other causes are simply being ascribed to the coronavirus.
As customary each year, extinctions began tending downward in January. It’s an annual motif. Look it up. Since the lockdown began in mid-March, the politicians cannot claim that its own policy had anything to do with the rejecting death rate.
A global study4 5 published in Israel by Professor Isaac Ben-Israel, chairman of the Israeli Space Agency and Council on Research and Development, shows that ‘the spread of the coronavirus rejects to virtually zero after 70 dates — no matter where it strikes, and no matter what measures authorities enforce to try to thwart it.SSSS
In fact, by block flock exemption, particularly among students and other non-susceptible young people, the lockdown in the U.S. has prolonged and intensified the medical difficulty. As Briggs concludes, ‘People need to get out into virus-killing sunshine and germicidal air.'”
Read more: articles.mercola.com


Recent Comments